Penile Curvature: Peyronie’s Disease – Diagnosis & treatment
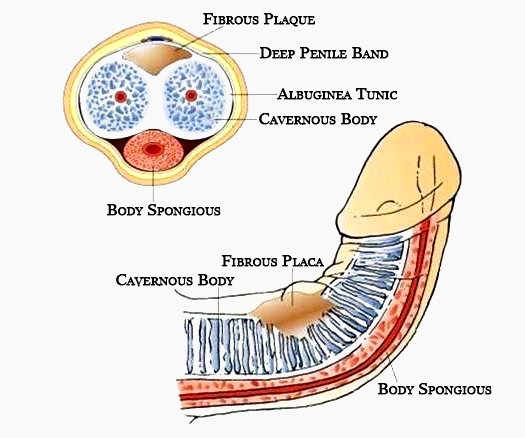
The Peyronie’s disease is characterized by the chronic inflammation of the Tunica Albuginea, a membrane that covers the corpus cavernosum of the penis.
The Tunica Albuginea is usually elastic and allows an elongation of approximately 30% of the length of the penis’ size when erect. In Induratio penis plastica, the penis becomes thickened, inelastic and sometimes hard and calcified.
In the initial phase, the hardening of the tissues is limited to small nodules, in later stages the nodules can multiply and extend to the majority of the penis.
This disease has the highest incidence on males between 50 and 65 years of age, but can also appear at an earlier age. Quite frequently, it is accompanied by diabetes, gout, hypertension and atherosclerosis. It can also be triggered by past events of traumas or microtraumas occurred to the penis; sometimes it can be triggered by injuries occurred during sexual activity. The disease is most frequently found in concurrence with other connective tissue diseases (e.g.: Dupuytren’s disease or handheld fibrosis, ear cartilage fibrosis, tympanosclerosis, arthritis etc.). The key element of the disease is the appearance of the hardening zone(“plaque”) on the tunica albuginea (sheath) of the corpus cavernosum, ranging from a few mm to 2-3 cm. This causes some local tenderness that is accentuated during erection, during the touching, masturbation or sexual intercourse.
Quite promptly, it results into a bending of the penis at an angle of the curvature in correspondence to the plaque. The bending can be moderate, but in some cases, can be so severe that it makes the penetration difficult or impossible. Hardening of the area is indeed a cause of alarm for the patient (the main concern is to have a tumor), secondly, pain in the area is also a matter of concern as it can prevent sexual activities and subsequently cause aesthetic and functional problems. The most reliable pathogenetic hypothesis traces the beginning of the disease to a microtrauma of albuginea with a small fracture of the sheath.
The process of tissue repair involves the production of fibrous substance by specialized cells (fibroblasts) to “close the fracture”. This process does not stop and the production of the fibrous tissue continues determining the appearance of a plaque that is rigid, inextensible and perceptible to touch. Many therapies have been proposed but with little results. The only substance that can stop the disease seems to be Vitamin E.
However, the therapy of Iontophoresis with verapamil and corticosteroids is helpful. At an early stage of the disease, the patient experiences a feeling of moderate penile pain accentuated by the erection. An area of localized hardening (plaque, nodule) appears and the penis tends to curve in correspondence of the plaque. The pain spontaneously tends to subside, the size of the plaque stabilizes and the bending halts; but this is only an apparent spontaneous improvement.
Actually, with the involvement of the lateral wall of the cavernous, the penis can reach out to straighten but will lose some of its length, it is often accompanied narrowing or by the formation of new nodules. The capacity of obtaining an erection is gradually reduced until the stage of impotency, which may also become absolute; this is because the changes faced by the tunic coating of the corpora cavernosa interferes with the mechanism of seizure of the blood within them (erectile dysfunction “venous leak”). Over time, the plaque tends to calcify and the penis becomes shorter and thinner. These modifications occur with a devious trend, generally in the space of several months, sometimes even slower; but they may also occur at a rapid pace and with acute progression. Inevitably, deep psychological problems occur due to the progression of the disease, erection difficulties or even out of self-developed “shame” in showing a deformed penis to the sexual partner; the psychological distress can further amplify the problem of sexual functioning.
An examination performed by a specialist is the essential tool to detect this disease. Besides recognizing the plaque, the visit allows to estimate the elasticity index of the penis, that is, the ratio between its length while in erection and in the flaccid state. This ratio gives us information about the extension of induratio itself.
Ultrasound, however, has its own importance but is employed in order to get precise indications only, namely the test tells us whether there are calcifications inside a plaque and, above all, if it is associated with a drug-erection test (a pharmacologically induced erection conducted by injecting substances such as alprostadil into the penis) allows us to study the arterial and venous vascular system: the blood flow ending in the penis through the cavernous arteries and the flows of the outbound blood, also called the veno-occlusive mechanism. This investigation is of particular importance when planning a surgical treatment, as it lets the patient know if there are any risk factors for the decline in erection.
The induratio penis plastica is a benign non-tumoral lesion and may never become a tumor.
Surgery is reserved for cases where there is a penile curvature that makes relationships difficult.
Penile Curvature: Peyronie’s Disease – Diagnosis & treatment Medical Tourism Italy
Your health starts here
We understand your concerns: traveling to a different Country, undergoing such a delicate therapy, once you complete this form you will be contacted within a business day. You will find a team ready to answer all of your questions.
We have a strict policy about privacy and data usage:
We have a strict policy about privacy and data usage:
- We will only use your contact information to take care of your case.
- Your phone number or email address will not be shared with any third parties.
- You will speak with a prepared Personal Health Planner with whom you can be 100% honest and upfront about any problem you’re experiencing.
- It is, and it will always be, 100% free.
+39 339 239 7405
Talk with an Expert